

Trapped Ulnar Nerve: Causes, Symptoms, And Ergonomic Relief For Desk Work

Your ring and little fingers start tingling as you lean into the keyboard. You uncurl your elbow, shake your hand, and wonder, do I have an ulnar nerve trapped again? If you've felt that buzzing "funny bone" ache at your desk, you're not imagining it. This guide shows how to spot the problem early, dial in simple ergonomic fixes, and use well-designed tools to keep you comfortable and productive.
What The Ulnar Nerve Does—And How It Gets Trapped

The ulnar nerve carries sensation to your little finger and part of your ring finger and powers many small hand muscles that control precision grip and finger spread. When the ulnar nerve gets trapped, most often at the elbow, sometimes at the wrist, signals get noisy: numbness, tingling, weakness, and, if ignored, permanent changes. If you want a practical overview of early relief strategies, see this guide on ulnar nerve entrapment NHS exercises.
Common Entrapment Sites: Cubital Tunnel And Guyon's Canal
Key point: Most cases involve compression at the elbow: fewer at the wrist. At the elbow, the ulnar nerve passes through the cubital tunnel behind the "funny bone." Flexing the elbow tightens this space and can stretch the nerve. At the wrist, the nerve travels through Guyon's canal at the base of the palm: pressure from a hard edge, a cyst, or handlebar loading can compress it. Both sites can make the ulnar nerve trapped and irritable during desk work if posture and pressure aren't managed.
Early Versus Advanced Compression
Early compression is intermittent: pins-and-needles after long elbow flexion, a sleepy little finger, fleeting clumsiness. Advanced compression shows up as constant numbness, reduced grip, muscle wasting, and clawing of the ring and little fingers. Early recognition matters, intervening before weakness becomes fixed often prevents lasting loss of function. Sources: OrthoInfo, "Cubital Tunnel Syndrome," AAOS, 2022: "Guyon's Canal Syndrome," National Dictionary of Medicine.
Symptoms You’ll Notice At Your Desk

Desk symptoms usually follow a pattern: elbows bent, wrists cocked, pressure on hard edges, and then the zing. If your ulnar nerve is trapped, the fingerprint is specific to the ulnar side of the hand.
Sensory Changes In The Ring And Little Finger
Look for numbness, tingling, or burning on the little finger and the ulnar half of the ring finger. With elbow-based (cubital tunnel) problems, both palm and back of these fingers can be affected. Wrist-based (Guyon's canal) issues often spare the back of the fingers and focus on the palm side. If these sensations appear after long typing, mousing, or phone scrolling with bent elbows, your ulnar nerve may be getting trapped by posture and pressure.
Grip Weakness And Fine Motor Difficulty
Notice subtle drops: missed key presses, trouble opening jars, shaky pinch when you grasp a cable or stylus. The ulnar nerve powers intrinsic hand muscles that stabilize fine movements. When compressed, grip strength fades and accuracy slips, especially late in the day when fatigue sets in and form breaks down.
Red Flags That Warrant Prompt Care
Constant numbness that doesn't fade, visible hand muscle hollowing, finger clawing, or sudden symptoms after a bang to the elbow or wrist need timely medical evaluation. These signs suggest more advanced or complicated entrapment. Don't wait, early treatment can protect function.
Desk And Lifestyle Factors That Raise Risk

The fastest way to aggravate an ulnar nerve trapped at the elbow or wrist is a repeat loop of flexion and pressure. Small choices, how you lean, where you rest, how far you reach, add up over a long day.
Elbow Flexion And Hard Desk-Edge Pressure
Bent elbows tension the nerve: direct pressure on the inner elbow amplifies it. Leaning on hard armrests or a sharp desk edge while you type or hold your phone can irritate the cubital tunnel. Keep elbows more open, and keep the "funny bone" off hard edges.
Wrist Deviation, Reach, and Contact Stress
Working with the wrist bent toward the little finger or extended while gripping a tall mouse narrows spaces at the wrist. Reaching far for a mouse or resting the palm on a narrow pad can increase pressure over Guyon's canal. Shorten the reach, center the device, and avoid hard contact on the ulnar side of the palm. A deeper look at device choice is covered in this guide to the best mouse for ulnar nerve pain.
Repetition, Force, And Vibration Exposure
High repetition with forceful gripping increases tissue bulk around the nerve. Vibration from cycling or tools can irritate nerve tissue and is linked to wrist-level compression (so‑called "handlebar palsy"). Keep grip light, vary tasks, and reduce vibration when possible.
Self-Care And Ergonomic Fixes That Help

Start with posture and pressure. Most desk-related cases improve when you open the elbows, keep wrists neutral, and remove sharp contact points. Layer in better device placement and short, regular movement breaks.
Neutral Elbows And Wrists With No Edge Pressure
Lead move: open the elbows. Aim for a relaxed, near‑straight angle while typing and mousing. Keep wrists neutral, no prolonged extension, flexion, or side bend toward the little finger. Add soft armrest or desk-edge padding so the inner elbow and the ulnar side of the palm never rest on a hard line. Less edge contact, less irritation to an ulnar nerve trapped by posture.
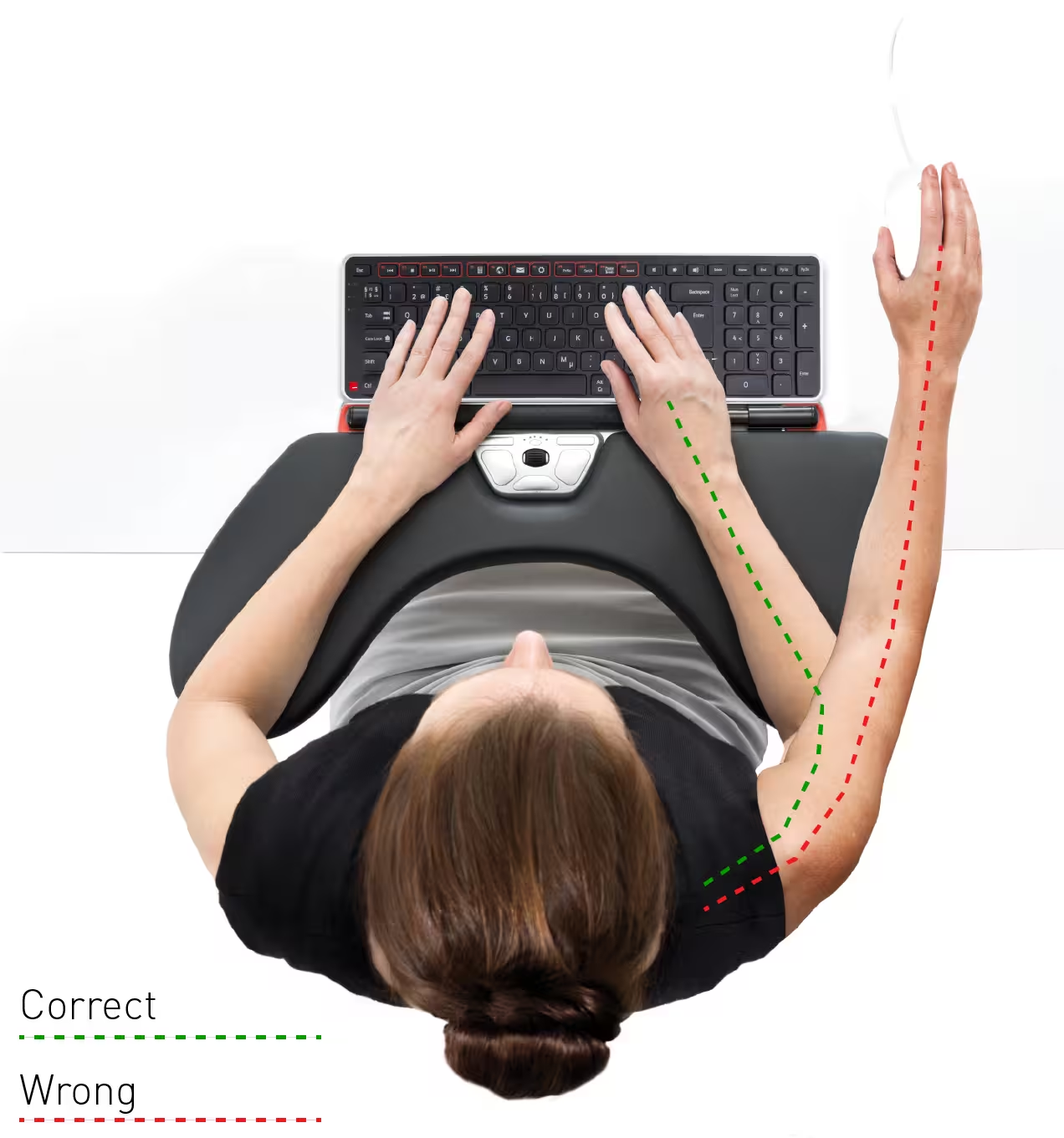
Centered Pointing And A Shorter Reach
Place your pointing device close to the spacebar, not out to the side. Central pointing removes long reaches and awkward wrist angles. Contour Devices® RollerMouse puts the control bar in front of the keyboard, no reaching, twisting, or gripping, so elbows stay open and wrists stay neutral. The SliderMouse Pro offers touchpad-like control with a low profile that supports a flat, relaxed wrist.
Keyboard, Mouse, And Palm Support Setup
A low-profile keyboard with slight negative tilt helps keep wrists straight. Contour's Balance Keyboard pairs clean lines with a compact layout so your mouse, RollerMouse, or SliderMouse can sit close. If you use palm support, choose broad, soft surfaces and rest lightly on the heel, not the ulnar edge of the palm. The UniMouse lets you adjust angle and thumb support, reducing the need to cock the wrist.
Microbreaks, Stretching, And Nerve Glides
Schedule 30–60 second breaks every 20–30 minutes. Straighten elbows, gently move wrists through comfortable range, and shake out the hands. Some clinicians teach ulnar nerve glides: learn them from a qualified provider so you mobilize without over‑stretching. Short, frequent movement reduces intermittent compression and helps an irritated ulnar nerve calm down.
Night Positioning And Light Splinting
Many of us sleep with elbows tightly bent. Keep them more open at night with a soft towel wrap or a light splint. This simple change can cut down on nocturnal tingling and morning numbness if your ulnar nerve is trapped at the elbow.
Diagnosis And Medical Treatment Options

If symptoms persist, a medical assessment clarifies where the nerve is compressed and how severe it is. Early diagnosis plus ergonomic changes often avoids surgery.
Physical Exam And Provocation Tests
Clinicians test sensation on the ulnar digits, check small-hand muscle strength, and look for atrophy or finger clawing. They may tap over the nerve (Tinel's sign) or hold your elbow in flexion to reproduce symptoms. These findings help distinguish elbow from wrist entrapment.
Nerve Conduction Studies And Ultrasound
Nerve conduction and EMG can show slowed signal across the elbow or wrist and grade the severity. Ultrasound can visualize swelling, snapping, or compression: MRI can reveal structural causes like cysts. Together, these tools localize the site so treatment fits the problem.
Conservative Care: Activity Changes, Padding, Medication
First-line care usually includes activity modification, padding or bracing (especially at night), and short courses of anti‑inflammatory medication when appropriate. Supervised therapy focuses on posture, nerve mobility, and habits that reduce pressure.
Injections, Surgical Options, And Recovery Timelines
In select cases, clinicians may consider targeted injections around inflamed tissue, used cautiously near nerves. If significant weakness or persistent numbness remains, surgery can decompress the cubital tunnel or Guyon's canal, sometimes moving the nerve (transposition). Wounds heal in weeks: nerve recovery often takes months. Reference: "Entrapment Neuropathies," American Family Physician, 2020.
Prevention For Individuals And Teams
Prevention is a daily practice: neutral joints, minimal pressure, frequent small resets, and the right tools within easy reach.
Workstation Standards And Procurement Considerations
For teams, specify adjustable chairs, sit‑stand desks, and arm supports that eliminate elbow-edge pressure. Choose low-profile keyboards and central pointing devices that reduce reach. Contour's RollerMouse and SliderMouse Pro support neutral alignment for diverse users, which simplifies ergonomic compliance across a fleet. Fewer complaints, fewer sick days.
Training, Monitoring, And Sustainable Equipment Choices
Provide quick training on early symptoms, posture, and microbreaks. Track discomfort reports and adjust equipment when patterns emerge. Opt for durable, repairable gear: Contour offers long-life devices and a Refurbished program that's better for budgets and the planet. See Balance Keyboard and RollerMouse Red for compact typing and centered control that help keep the ulnar nerve untrapped during long projects.
Conclusion
Comfort shouldn't be optional. If you've felt your ulnar nerve trapped by long hours, start small today: open your elbows, clear the edges, center your pointing, and take microbreaks. Then choose devices that match the way you work, RollerMouse or SliderMouse Pro for centered control, UniMouse for adjustable angles, Balance Keyboard for neutral wrists. Say goodbye to feeling sick, strained, and sore. Contour Devices. Work miracles.
This article is general information and not medical advice. Seek clinical care for diagnosis or treatment, especially if you notice constant numbness, weakness, or deformity.
Key Takeaways
- Recognize the fingerprint of an ulnar nerve trapped: tingling or numbness in the little and ring fingers that worsens with elbow flexion—act early to prevent lasting weakness.
- Open your elbows, keep wrists neutral, and avoid hard desk‑edge pressure to calm compression at the cubital tunnel or Guyon’s canal.
- Center your pointing device and shorten reach; consider central pointing solutions and low‑profile keyboards to maintain neutral alignment and reduce strain.
- Take 30–60 second microbreaks every 20–30 minutes, move wrists gently, and perform clinician‑taught ulnar nerve glides without overstretching.
- Seek prompt care for constant numbness, visible muscle wasting, or finger clawing, which signal advanced entrapment.
- If symptoms persist, clinicians can localize the site with exam and nerve studies, start conservative care, and reserve surgery for persistent deficits.
Ulnar Nerve Entrapment: Frequently Asked Questions
What does it mean to have the ulnar nerve trapped, and where does it usually happen?
An ulnar nerve trapped typically refers to compression at the elbow (cubital tunnel) or less commonly at the wrist (Guyon’s canal). It causes tingling or numbness in the little finger and half of the ring finger, grip weakness, and clumsiness—often worse with prolonged elbow bending or pressure on hard edges.
Which desk habits aggravate ulnar nerve entrapment symptoms?
Common culprits include elbows bent tightly, leaning on the inner elbow or sharp desk edges, reaching far for a mouse, cocked wrists, and resting the ulnar side of the palm on hard surfaces. High repetition, forceful gripping, and vibration exposure can further irritate the nerve, especially during long work sessions.
How can I fix an ulnar nerve trapped at my desk without surgery?
Open your elbows and keep wrists neutral, add soft padding to avoid edge pressure, and place the pointing device centrally to shorten reach. Use low‑profile keyboards, broad palm supports, and take 30–60‑second microbreaks every 20–30 minutes. Nighttime elbow wrapping or light splinting and clinician‑taught nerve glides may help.
When should I see a doctor for ulnar nerve symptoms?
Seek prompt care for constant numbness, visible hand muscle hollowing, finger clawing, or symptoms after trauma. Clinicians may perform sensation and strength tests, provoke symptoms with elbow flexion or Tinel’s sign, and use nerve conduction studies or ultrasound to localize compression and guide treatment.
How is ulnar nerve entrapment different from carpal tunnel syndrome?
Ulnar entrapment affects the little finger and half of the ring finger, often worsens with elbow flexion, and can cause intrinsic hand weakness. Carpal tunnel involves the median nerve—thumb, index, middle fingers—with thenar weakness and nocturnal numbness. Tests and exam location help distinguish them for targeted treatment.
How long does recovery take for an ulnar nerve trapped condition?
With activity changes, padding, and night splinting, mild cases often improve over 6–12 weeks, though nerve irritability can take several months to fully settle. After surgical decompression, wounds heal in weeks, but nerve recovery commonly progresses over months, sometimes up to a year, depending on severity and site.
